Objectives
Advanced Life Support Algorithm
 The Advanced Life Support (ALS) algorithm provides a standardised approach to the management of a person experiencing cardiac arrest which enables treatments to be expediently executed without the need for protracted discussion. The algorithm is divided into two pathways, one pathway for shockable rhythms (VF/pVT) and the other pathway for non-shockable rhythms (PEA/asystole).
The Advanced Life Support (ALS) algorithm provides a standardised approach to the management of a person experiencing cardiac arrest which enables treatments to be expediently executed without the need for protracted discussion. The algorithm is divided into two pathways, one pathway for shockable rhythms (VF/pVT) and the other pathway for non-shockable rhythms (PEA/asystole).
The main difference in the management between the two pathways is the need for defibrillation for patients presenting in VF or pulseless VT. Other interventions such as high-quality chest compressions with minimal interruptions, airway management and ventilation with 100% oxygen (O2) when available, intravenous or intraosseous access, administration of adrenaline every 3 – 5 minutes and the early identification and correction of potentially reversible causes, are common to both pathways. Soar et al, 2021, Resuscitation, p125; ANZCOR Guideline 11.2, 2021
Note… Interventions that have unquestionably increased survival post cardiac arrest are uninterrupted high quality CPR and early defibrillation. Monsieurs et al, 2015 p17; ANZCOR Guideline 11.2, 2021
Finding a cause
The management of sudden ventricular fibrillation or pulseless ventricular tachycardia (VF/pVT) arrests is relatively straightforward. In these cases management consists of maintaining coronary perfusion with basic life support and instigating early defibrillation. These measures may be successful at reverting the arrhythmia without any other intervention, and without knowing the cause of the arrhythmia. The majority of cardiac arrest survivors come from VF/pVT arrest.
If VF or pVT are not present, thus the patient is experiencing a non-shockable arrest (pulseless electrical activity or asystole), it is important to find and treat the cause of the arrest as quickly as possible. A useful memory tool to recall the conditions that may lead to cardiac arrest are the four Hs and four Ts. Assessing for the presence of these conditions, followed by appropriate treatment in a timely manner, are the critical components of a successful resuscitation.
Did you know… In adult cardiac arrests, on initial monitoring only about 20% of cardiac arrests present in a shockable rhythm, thus 80% are not shockable. The incidence of VF/pVT may be decreasing. Soar et al, 2021 Resuscitation, p125
Potential causes of cardiopulmonary arrest
Did you know… Cellular oxygen consumption decreases by about 6-7% per 1oC drop in core temperature. At 18oC the human brain can tolerate cardiac arrest up to 10 times longer than at 37oC. Lott et al, 2021, p180; Monsieurs et al, 2015 p22
Soar et al, 2021, Resuscitation, ANZCOR Guideline 11.2, 2021
Correcting Reversible Causes
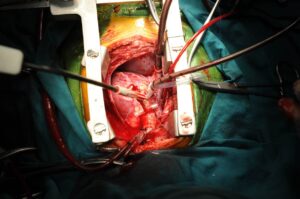
 In order for a rescuer to determine and correct potentially reversible causes of cardiac arrest an evaluation of the physical circumstances of the arrest, precipitating factors and clinical examination as well as the use of adjuncts (e.g. ultrasound) will be required. The rescuer should undertake interventions based on the presumed aetiology of the arrest (i.e. cardiac or non-cardiac).
In order for a rescuer to determine and correct potentially reversible causes of cardiac arrest an evaluation of the physical circumstances of the arrest, precipitating factors and clinical examination as well as the use of adjuncts (e.g. ultrasound) will be required. The rescuer should undertake interventions based on the presumed aetiology of the arrest (i.e. cardiac or non-cardiac).
Knowledge of the potential causes of arrest and the pathophysiology associated with each cause will support effective and efficient treatment for the victim and enhance the possibility of successful outcome.
Remember… High quality CPR with minimal interruption and treatment of reversible causes are the most important interventions in cardiac arrest. ARC Guideline 11.10, 2021
Adult Advanced Life Support Protocols
Continue high quality chest compressions, with 100% oxygen if available, until defibrillator arrives. As soon as defibrillator is present, apply self-adhesive defibrillation pads whilst chest compressions continue, then pause briefly (no more than 5 seconds) to analyse the rhythm. If a shockable rhythm is present follow the shockable pathway of the algorithm; should a non-shockable rhythm be present and there is no sign of spontaneous circulation, follow the non-shockable pathway. Soar et al, 2021, Resuscitation
Important note…..
Some courses instruct to charge defibrillator towards the end of every 2 minute cycle of CPR in preparation for rhythm analysis/pulse check which is consistent with ANZCOR guidelines. If VF or pulseless VT is present the shock is given, if a non-shockable rhythm is present the defibrillator is disarmed or left to disarm (this approach may be well suited to critical care units). The benefit of this approach is unknown. A study conducted by Cheskes et el, “Compressions during defibrillator charging” (2014) found ‘there was no significant difference between the compressions during charging study group and the no compressions during charging group with respect to Utstein variables’, and clinical outcomes (ROSC or survival) did not differ between the two approaches. Should the defibrillator be left to disarm this will take about 1 minute, and if the defibrillator is charged again before the next rhythm check, results in the defibrillator being charged for the majority of the time during the resuscitation attempt. In addition, this approach results in the defibrillator being charged for non-shockable rhythms and has resulted in inadvertent shocks being delivered. (Sour et al, 2015, p106) Should a non-shockable rhythm with low output be inadvertently defibrillated, VF could be initiated when all that was needed was some short term compressions to assist with perfusion. Further, should the victim be in a non-shockable rhythm and haemorrhaging, repeated charging of the defibrillator results in unwarranted hands off wound time until the defibrillator is disarmed. Defibrillators have different functions to disarm the charge and anecdotal evidence suggests clinicians are unfamiliar with the procedure to disarm the defibrillator, despite training. As the majority of cardiac arrests are not shockable and to cater for a variety of diverse cardiac arrest responders and situations, this course instructs brief rhythm analysis (<5 seconds), then if VF/pVT is identified, chest compressions are continued while the defibrillator is charged. Vital emphasis on minimal interruption to chest compressions and early defibrillation is maintained (this is in-line with the European Resuscitation Guidelines and is also consistent with paramedic/medic protocols). Briefly pausing compressions (<5 seconds) to analyse rhythm on initial monitoring has not been shown to adversely affect ROSC, avoids repeated charging of the defibrillator for non-shockable rhythms, and enables translation of training to specific cardiac arrest situations such as traumatic cardiac arrest as well as arrests occurring in operating theatres, in-flight and in rural settings. (Sour et al, 2015)